





CLASSIC & LASER MASTOPEXY (BREAST LIFTING)

Mastopexy, also known as breast lift surgery, is a surgical procedure that gives breasts a more youthful appearance by removing lax skin, shifting the nipple upward, and redistributing tissue to achieve the desired shape.
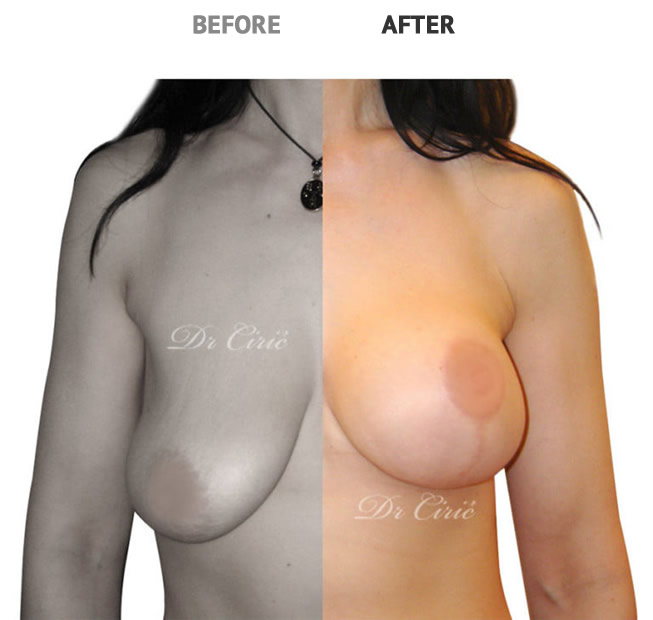
Pregnancy, lactation and the force of gravity over the years affect the appearance of women’s breasts. Laser Mastopexy is a surgical procedure which lift and shape drooping breasts.
If the cut is performed with a scalpel it is a classic operation, if it is create with a laser – it is the laser surgery.

Inverted T / Anchor Mastopexy Technique
The type of breast lift scar a woman winds up with depends on several factors, and there’s no standard protocol or formula when it comes to mastopexy.

Historically, the most commonly used technique for managing the redundant skin envelope in mastopexy was the Wise pattern inverted T approach. As a result, it is this technique against which all other ‘short scar’ techniques are measured in terms of results and complications. Here, the apex of the inverted T is located by transposing the inframammary fold anteriorly onto the breast by placing the fingers of the left hand under the breast and palpating with the right hand where the tips of the fingers could be felt. An angled inverted V pattern is then drawn from this point downward, skirting the medial and lateral margins of the areola with the lengths of these two limbs being 5–7 cm long. A medial and lateral extension is then drawn as needed to meet a similar line drawn directly in the inframammary fold. The strategy of this marking pattern is to keep the inframammary component of the incision as short as possible to appropriately take up any redundancy in the skin pattern and yet not leave behind a ‘dog ear’ at either the medial or lateral end of the incision. After the breast is re-shaped, the areola is then inset into a matching defect created by removing a circular segment of skin at the apex of the vertical incision. The advantage afforded by this technique relates to the ease with which the skin envelope can be reduced as even large skin redundancies can be managed without difficulty. Because of the manner in which the pattern is designed, there is a more or less 1:1 relationship in the lengths of the corresponding skin incisions, which eases closure and prevents any of the pleating or skin redundancy that can be noted with periareolar or circumvertical techniques. Because of the familiarity many surgeons have with the inverted T technique along with the directness of the skin closure, this pattern remains a popular choice for mastopexy.
It must be noted that the major drawback associated with the Wise pattern technique is the presence of the inframammary scar. For patients who are approaching their mastopexy procedure with an aesthetic mindset, the presence of this scar can be quite objectionable and many patients who are otherwise excellent candidates for a breast-lifting procedure will decline based on concerns related to the scar. Therefore, although the pattern is well suited for the treatment of macromastia where the dimensions of the skin envelope tend to be more substantial, in my opinion, this skin management strategy is overly aggressive when applied to mastopexy. The same goals can be reached using periareolar and circumvertical techniques with a reduced scar burden for the patient. For this reason, the inverted T skin pattern is used only in special circumstances where previous scars or other sequelae from previous surgery make short scar techniques less predictable.
Mastopexy and Augmented Mastopexy
Mastopexy is indicated for severe ptosis of the breasts without volume loss; an augmented mastopexy is indicated when ptosis is associated with volume loss. Bilateral midclavicular lines and the inframammary fold are marked with the patient in standing position. The proposed site of the neoposition of the nipple-areola complex is just above the inframammary fold.
The patient is in the supine position, under general anesthesia. The staple test is carried out. Marchac’s modification of the Lejour vertical mastopexy is based on the central pedicle.6 Tumescent infiltration is carried out, followed by the skin excision. Transposition of the nipple-areola complex on the central glandular pedicle is done.
Vertical closure with minimal horizontal extension as described by Lejour and modified by Marchac is completed.6 Skin closure is done with 3-0 and 5-0 Monocryl sutures; the patient should wear a sports bra.
With age, breasts once perky and full begin to deflate and droop. Creams do very little to help, and exercise can make the problem even worse. Breast lift surgery is the only truly effective solution — if you can deal with the scars.
Mastopexy, also known as breast lift surgery, is a surgical procedure that gives breasts a more youthful appearance by removing lax skin, shifting the nipple upward, and redistributing tissue to achieve the desired shape.
While this may sound like the perfect way to turn back the hands of time, there’s a trade-off – scars.
Plastic surgeons are quick to point out that breast lift scars fade over time, and while most women recognize that even the nastiest post-op scar can be covered with the right undergarments or swimsuits, that’s cold comfort to those who want to look great naked.
It’s not all bad news though. Certain surgical techniques result in less scarring, and proper postoperative care can dramatically minimize the appearance of scars. Here are your options.
The type of breast lift scar a woman winds up with depends on several factors, and there’s no standard protocol or formula when it comes to mastopexy.

Breast lift techniques
When discussing your concerns with your surgeon, it is important to mention what type of scarring is acceptable to you. While all breast lift procedures have a level of scarring, certain techniques aim to mask the scars in various ways.
Breast lift techniques tend to go by names that reference the shape of the scars that they leave behind. These include:
• The crescent lift
• The donut lift
• The lollipop lift
• The anchor lift
• The horizontal mastopexy
• The “scarless” lift
Each technique comes with its own set of advantages and disadvantages, and no option is the best for all patients. It is important to choose the lift that best meets your aesthetic goals.
The crescent lift
The crescent lift gets its name from the crescent shaped skin above the areola that is excised during the procedure. When the skin edges are sutured closed, the nipple is raised by a few centimeters.
It’s a popular method because the incision enables doctors to reshape breast tissue and insert implants either above or below the muscle, leaving only a small scar along the top of the areola. However, it also has its downsides: only a minimal amount of lift can be achieved, not all sizes and types of implants will fit, and the majority of women desire a bigger boost than this method can deliver.
The donut lift
Another popular technique to elevate the breast involves a periareolar incision, also known as a donut lift due to the shape of the skin removed during surgery.
With this procedure, a surgeon creates an incision on or around the perimeter of the areola and later a second outer incision to remove the “donut” of skin around it. The nipple is sutured back to the breast skin, tightening it in the process. This method provides more lift than the crescent, but again only a relatively small amount of sagging can be repaired.
The lollipop lift
For women with more sagging than can be corrected through the crescent or donut methods, doctors may opt to perform a lollipop lift.
Also known as a vertical lift, this technique requires surgeons to make a keyhole shaped incision on the breast, preserving the nipple but removing any excess skin below it. The areola is then shifted up into its new position, while suturing the skin edges together results in a lollipop shaped scar around the nipple and a vertical line down to the breast crease.
The anchor lift
Then there is the anchor lift (or inverted T). It’s the oldest mastopexy technique, considered by many surgeons to be the “gold standard” for women with severe ptosis requiring a significant amount of skin to be removed in order to achieve a perkier shape. It’s also the most invasive method and leaves the largest scar.
To shift the nipple upward, doctors create an incision around the areola and under the breast crease. A portion of skin is removed from under the nipple, which is then raised to a higher position. Closing the incisions leaves an anchor-shaped scar that follows the curve of the breast.
Surgeons may also combine or alter these techniques during modified vertical lifts which will leave “J-shaped” or “inverted short T -shaped” scars.
The horizontal mastopexy
The horizontal mastopexy goes by many names, including the “Horndesky Method” and “Ultimate Lift.” This technique enables surgeons to create a new position for the nipple without leaving a vertical scar from the areola to the breast crease. Instead, a horizontal incision is made across the entire breast above the areola, and the surgeon excises the skin below it while preserving the nipple.
The nipple is then pulled through a new round incision higher up on the breast, and when the incisions are sutured closed, the patient is only left with horizontal scars on the breast crease and around the areola.
Although the oft-dreaded vertical scar is avoided, the trade off is the final shape of the breast could wind up being more boxy than round, and the sutures may result in a puckering of the skin along the breast crease.
The scarless lift
Finally, there’s the so-called scarless lift. Women who are seeking a mild lift but are dead set against leaving scars anywhere on their breasts may opt for a technique that uses a network of dissolving surgical threads inserted through tiny incisions along the collar bone, guided under the breast tissue, and then anchored to the collar bone, to create an internal bra of sorts. Scar tissue forms around the threads, theoretically providing support to lift the nipple.
Technically, this method still leaves scars along the collarbone, but they’re tiny. It’s also considered by many to be the least invasive of breast lifts, but it’s also the least effective, and most women won’t even be a candidate for this option.
Unfortunately, selecting the right technique for your mastopexy isn’t as simple as ordering off a menu. The type of scar a woman winds up with depends on the type of surgery she needs, and there’s no standard protocol or formula when it comes to mastopexy.
The clinic is equipped with latest technology that is applied around the world. Behind the staff of our clinic is over 42 years of international experience in medicine and surgery.
Show us your trust, call us, and we will do everything to make you happy with your new look.
More information about the treatments can be obtained: Online Contact Form – Go to the page
Viber / WhatsApp +381 65 30 66 989
PRICE LIST BREAST LIFTING
Breast lifting (tightening) – standard – from 4500
Breast lift (tightening) with implants without correction of excess skin from 4500
Breast lifting (tightening) – with single laser – from 5000
Breast lifting (tightening) – with combo laser C02/NdYAg – from 6500
* Important Note:
Prices in the price list are approximate. The final price after examination and consultation with the surgeon.
Prices are expressed in EUR, payment in dinars at the Bank Intesa sales rate on the day of payment.